{kind=link}
TLDR: The current advice that LDL is “bad cholesterol”, appears to be outdated, and the actual situation is more complex. In people over 60 high LDL appeared to be protective for mortality.
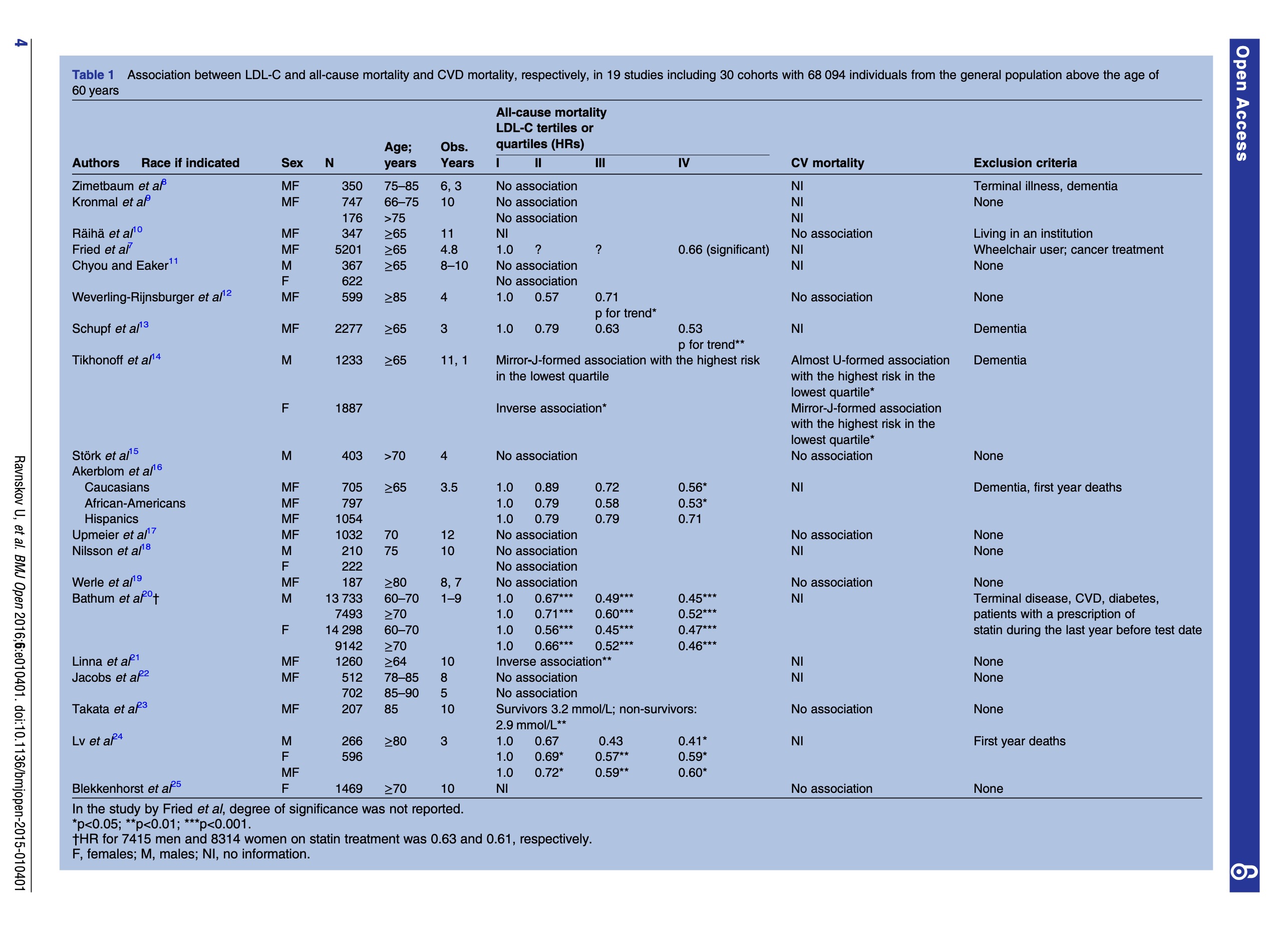
Conclusions: High LDL-C is inversely associated with mortality in most people over 60 years. This finding is inconsistent with the cholesterol hypothesis (ie, that cholesterol, particularly LDL-C, is inherently atherogenic). Since elderly people with high LDL-C live as long or longer than those with low LDL-C, our analysis provides reason to question the validity of the cholesterol hypothesis. Moreover, our study provides the rationale for a re-evaluation of guidelines recommending pharmacological reduction of LDL-C in the elderly as a component of cardiovascular disease prevention strategies.
Full Paper at https://pubmed.ncbi.nlm.nih.gov/27292972/
Related to, and following up on the LMHR paper from https://hackertalks.com/post/5835924
So, any doctor that just looks at LDL and says “number high, you take statin” needs to be roundly shamed and sent off to the reeducation camps. This has not been the consensus for decades and modern risk stratification tools generally don’t even take into account LDL and instead use a HDL/Total chol ratio.
What is uncontroversial is that statins reduce risk in people who are already at moderate to high risk of cardiovascular events, ideally initially with risk stratification tools like ascvd and followed up with coronary artery calcium scoring or angiography if required.
For FH in particular statins do dramatically reduce risk of CV events.
20-Year Follow-up of Statins in Children with Familial Hypercholesterolemia NB. The children took statins, their parents didn’t.
Your doctor may know all this or they may be a quack who is right by accident. I’d guess the former, I’ve been a doctor for a decade and was taught the above in medical school.
@[email protected]
Really well said!
I thought the TG/HDL ratio was the gold standard now. I.e. https://hackertalks.com/post/5922188
Looks like that paper is looking at TG/HDL as a marker for insulin sensitivity and MetSy which is a related but distinct kettle of fish.
I read the paper, thanks for the link! I found it interesting.
The paper doesn’t make it clear if this is a statement with respect to FH, or humans in general. One caveat that comes to mind is this statement is lumping in all types of LDL
From the introduction of the paper, they define FH as miscoded lipoproteins. I’m not sure the LDL in FH is compatible to non-miscoded LDL (normal people, not glycated, or oxidized), at least in so far as making the first statement a “fact”
From Non-coronary heart disease mortality and risk of fatal cancer in patients with treated heterozygous familial hypercholesterolaemia: a prospective registry study - Full paper is on scihub
Admittedly this study is 10 years older
table 3
Table 5 is also really interesting.
After statin availability subjects with FH appear to have less cancers then the general population. I wonder if this suggests that while very high LDL can be a CVD risk factor, could it also be a cancer risk factor? The authors suggest the cancer reduction is due to lifestyle advice given, but I think it could be suggestive of a impact of LDL. Or was the elevated LDL while being treated with statins protective?